Gilligan’s Guide
Gilligan’s Guide is an algorithm (a graphic chart that is easy to follow) which assists the pregnant person’s body to rotate their unborn infant into the optimal or best position for birth. We refer to this as “Maternal Positioning for Optimal Fetal Positioning”. It is safe, simple and efficient for everyone to use. Please, always consult your provider before using the Guide. Since I am a Registered Nurse, safety is always the first thing on my mind. I am also recommending that you use a doptone or an external fetal monitor to monitor the infant’s heart rate when doing any type of maternal positioning.
Gilligan’s Guide will be provided to you on our first visit, accompanied by a full demonstration and explanations of each position and their benefits.
I am very proud of how the guide has come together with the help of all of my educational opportunities and my many mentors. If you are a member of the birth community; Physician, Nurse, CNM or doula, I would love to teach you personally, the anatomy and physiology behind Gilligan’s Guide. Special thanks to my thousands of clients who demonstrated great power and strength through their birth journeys, and Dr. Carol Phillips; Jean Sutton, PNM; Gail Tully, CPM; Rebecca Dekker, RN, PhD; Penny Simkin, PT; Jean Sutton, NM and Lisa Cook, RN, for their teachings.
“One of the most important aspects of a laboring primigravida (a woman who is pregnant for the first time) is the position of her infant in utero. We discuss dilitation, effacement and station, but ignore position. Remember, in relation to labor and delivery, there are four things that need to be addressed. Power (contractions), Passenger (infant), and Passage (pelvis), and Psyche (mental state). If we as caregivers, would put more emphasis on the Passenger, at term and in labor, the cesarean rate would fall.”
-Ann Gilligan, RN
What do I mean when I say malpresentation?
This website does not refer to the breech infant in respect to any aspect of Gilligan’s Guide. I am of the opinion that the relaxation of the lower uterine muscles will assist in the rotation of the infant into the head down or vertex position but you will have to visit other respectable websites such as Spinning Babies, in order to learn how to turn a breech.
The acronyms of the malpositioned infants are as follows:
ROT (Right Occiput Transverse): Infant’s spine is on the maternal right and the infant looking at the maternal left. When you look up at the maternal uterus, the heavy side will be on maternal right. Leopold’s maneuver will palpate the infant back on maternal right side.
ROA (Right Occiput Anterior): infant spine on maternal right but looking towards the maternal spine. Leopold’s maneuver will palpate infant’s back on maternal right just right of center.
OP (Occiput Posterior): infant’s spine will be against maternal spine, face looking up towards maternal belly button. Leopold’s maneuver will palpate small parts of infant on maternal belly. Many women have back labor with an occiput posterior infant.
Asynclitic: Vertex (head) of infant is not flexed and is often off to the maternal left or right. Leopold’s maneuver will palpate the infant in a non-straight up and down position. The woman might feel pain on one side of her body or back.
Why is the correct position for birth important?
Since 1997, the cesarean section rate in the U.S, per the CDC and NCHS, has increased 41%. Per ACOG, American College of Obstetricians and Gynecologists, the most common indications for primary cesarean delivery in order of frequency is; labor dystocia (a stall or cease in the dilitation of the cervix or the descent of the fetus), abnormal or indeterminate fetal heart rate tracing, fetal malpresentation, multiple gestation and suspected fetal macrosomia. Maternal positioning has been shown to improve the incidence of all of these except that of “multiple gestation.”
Malpresentation, especially that of OP, occiput posterior (looking at the stars, sunny side up), pose challenges in every aspect of intrapartum (during labor) care. Malpositioned infants are associated with labor abnormalities that may lead to adverse maternal and neonatal consequences. Therefore it is essential that the attempt be made through safe and effective maternal positioning in order to create a path to a more expedient, less painful and more satisfying delivery for every woman and fetus.
Why does the medical community not make this information available for all pregnant women?
My instructions have been enthusiastically accepted and incorporated into practice in my current world of obstetrics. I teach the new labor and delivery nurses, and have taught numerous classes for physicians, midwives and doulas. The testaments that I have heard as to why they were not aware of how to use maternal positioning and it’s benefits have all had similar reasonings such as the fact that they “were never taught this in school.” Once taken a class, they have walked away with a new tool to use with each and every patient. The anatomy and physiology of birth has never been so important as it is in 2020. As stated, I have been an obstetric nurse for 30 years and what I witness as far as the position of the infant in utero, today, is different from decades ago. My theory is that inactivity due to the increased use of computers and increased time driving, has led to many more infants who when term (37+ weeks) or in labor, are in a position less than optimal. So, unless we do something about this now, the cesarean rate and other co-morbidities (problems associated with an infant who is not in the optimal position for birth) will continue to rise. I am working furiously to change that and I need your help.
Are there medical studies that show that maternal positioning is safe and effective?
I am aware of very few formal medical studies that have been published in regards to the effectiveness of maternal positioning in labor. The few that I have found did not find evidence of an effect on the progress or outcome of labor. Interestingly, each of these studies, end with a statement that “further research is needed.” I can attest to hundreds of success stories associated with Gilligan’s Guide and would welcome any medical research made possible. The other aspect of these negative conclusions are the fact that none of the three I am aware of took into account what all of my advice is based on…..Passive stretch of the lower uterine support structures and a change in shape of the bony structures. Therefore, there is relaxation symmetry of the maternal pelvis and uterine supports which allow space for the infant to flex it’s head, and then rotate and position itself on the maternal left side. None of these studies applied this concept. Relaxation, Space, Flexion and Rotation is the reason why Gilligan’s Guide works.
Is there anything you can do to prevent a malpositioned once term or in labor?
Yes! Once seen and evaluated, I will come up with a plan for you to enhance the chances that your infant will be in the best position possible for birth. These can be as easy as sitting with your knees lower than your hips and avoiding the lounging position that is so common in today’s society. If you have an infant that has it’s back on your left side and it’s head tucked towards it’s chest, the chances of you having a spontaneous labor increases.
Is Gilligan’s Guide easy to do?
Yes! The best thing about Gilligan’s Guide is the ease in doing the positions and the the limited time that it takes to perform. Gilligan’s Guide is very safe for mother and baby. I am a registered nurse, therefore I am always thinking of safety first. There are some things listed on other sites that are not safe to do if you have certain conditions such as high blood pressure or polyhydramnios (increased amount of amniotic fluid). When developing this Guide, it was imperative that I considered all pregnant women, including those with medical conditions.
The Cardinal Movements of Birth



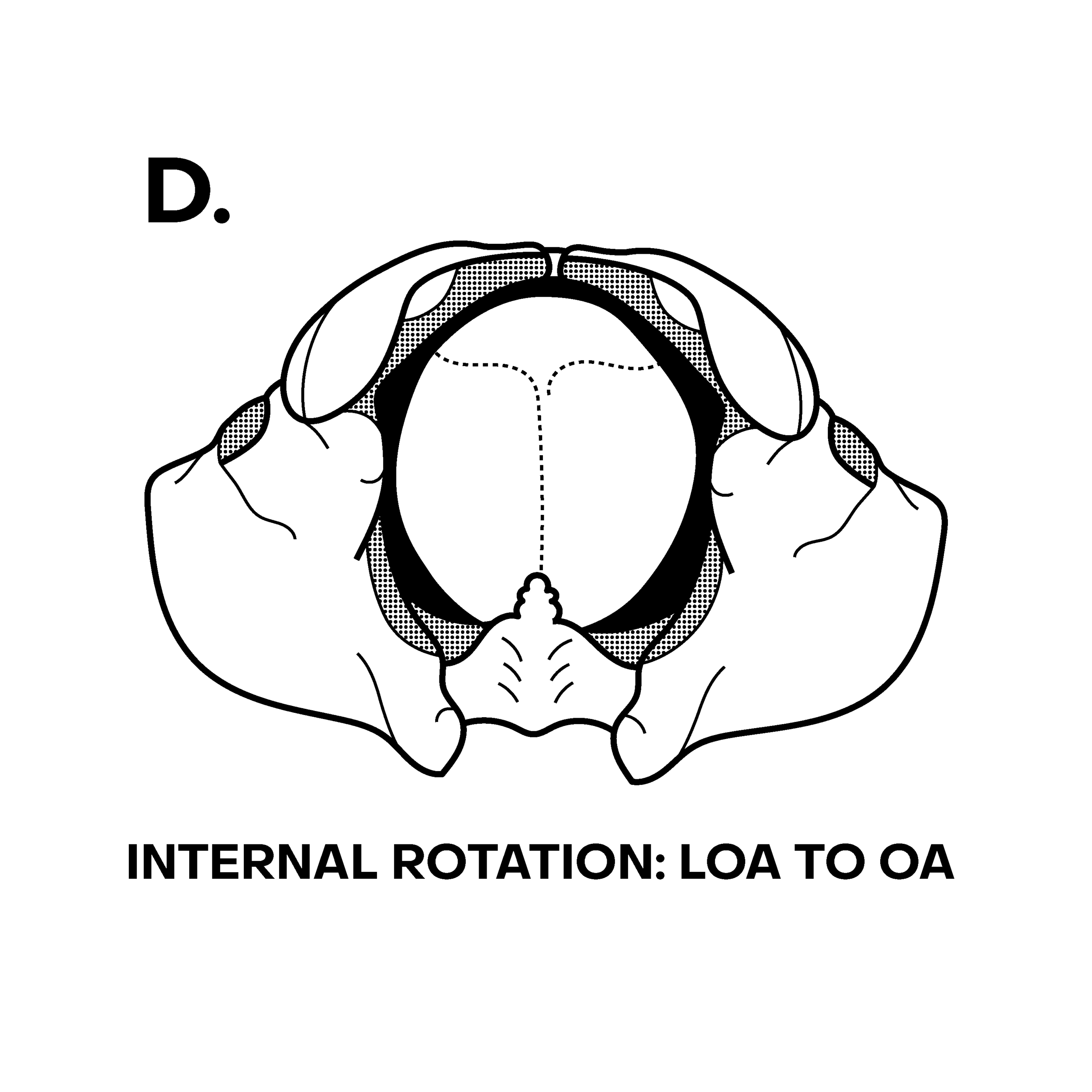

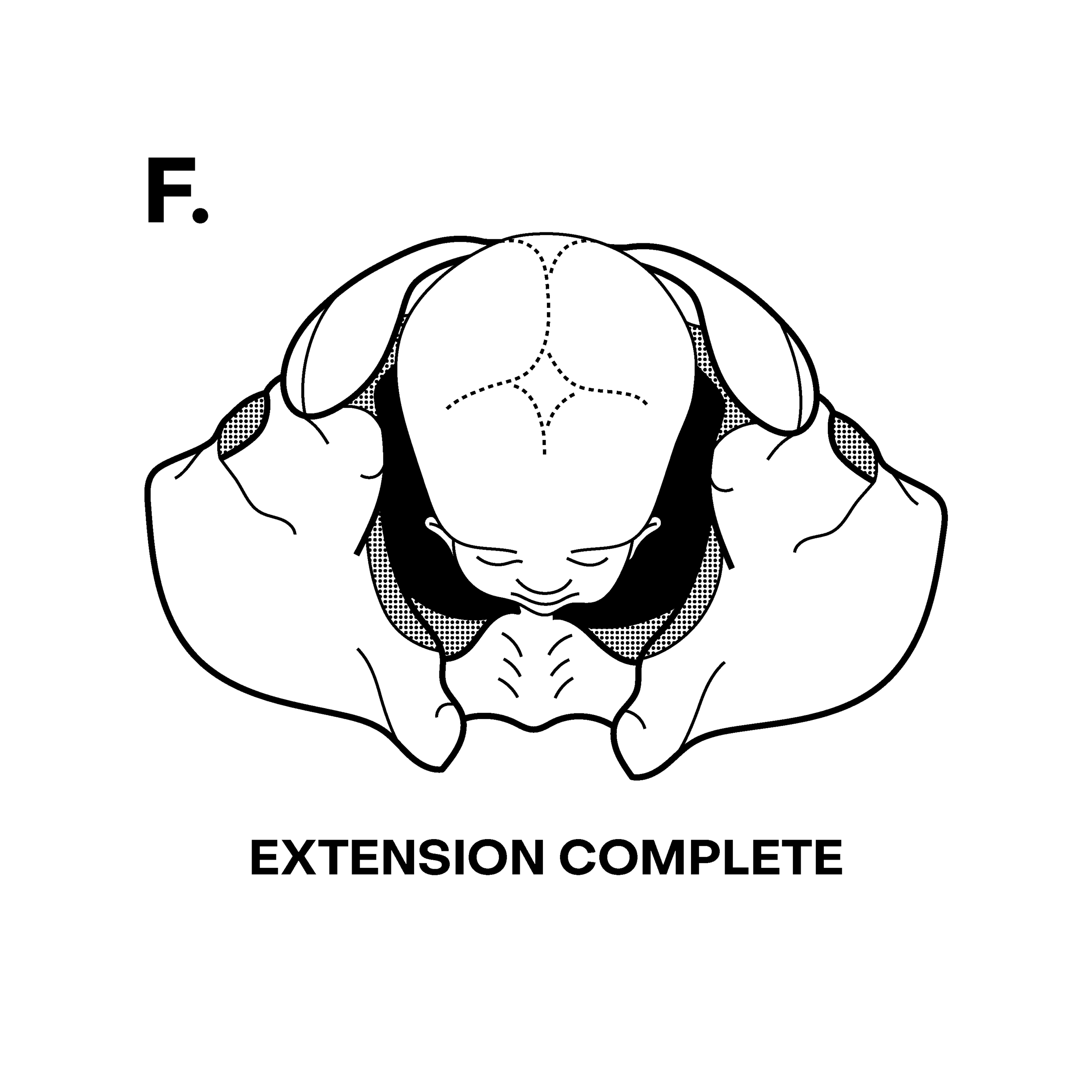



Fetal head
If the infant has it’s chin tucked toward it’s chest, there is less change to the shape of the head as the smallest diameter of the head, the occiput (back of the head) enters the inlet of the pelvis first. Gilligan’s Guide will assist in the process of “tucking of the chin.”

The Female Bony Pelvis
Gilligan’s Guide takes into account the ability of the bony pelvis to change shape and increase in size to accommodate the shape and size of the fetal head.